
After multiple overdoses, Bradley Ketcherside repeatedly applied for medically assisted treatment for his opioid use disorder while incarcerated at Crossroads Correctional Center. The first time, in October 2024, a far-off release date disqualified him for the medication, records show. Two months later, it was his placement in solitary confinement that barred him from treatment — even though drug use was what landed him in the hole.
On his final application in January 2025, a mental health evaluator recorded Ketcherside pleading that medication “would save my life.” The evaluator denied his request, according to medical records, concluding that Ketcherside didn’t show severe enough signs of addiction to require treatment.
Six days later Ketcherside was dead. Staff found him cold and unresponsive in his cell, according to a recently filed federal civil rights lawsuit on behalf of his widow. Medical providers attempted to administer Narcan, an opioid overdose reversal drug, but it was too late.
In a complaint filed on March 5, attorneys with the civil rights and immigration law firm Khazaeli Wyrsch allege the circumstances leading up to Ketcherside’s death are not an anomaly. Rather, the suit argues that the Missouri Department of Corrections and healthcare provider Centurion Health “systemically deny and unreasonably delay necessary medical care to inmates diagnosed with opioid use disorder,” discriminating against them and placing them at unnecessary risk of death.
In a prison system flooded with drugs, where staff play a role in smuggling illicit substances, Ketcherside’s death illustrates the department’s numerous failures to prevent overdoses among its prison population, the lawsuit alleges. Staff respond to overdoses with punishment and put up arbitrary barriers to drug treatment, denying people access for being sober for too long and also denying them when they use, lawyers allege.
“The stakes are life and death,” said Leah Fessler, lead attorney on the case. “ It is a huge injustice to allow people to die in prison from the condition that put them in prison without offering them any access to proper medical treatment.”
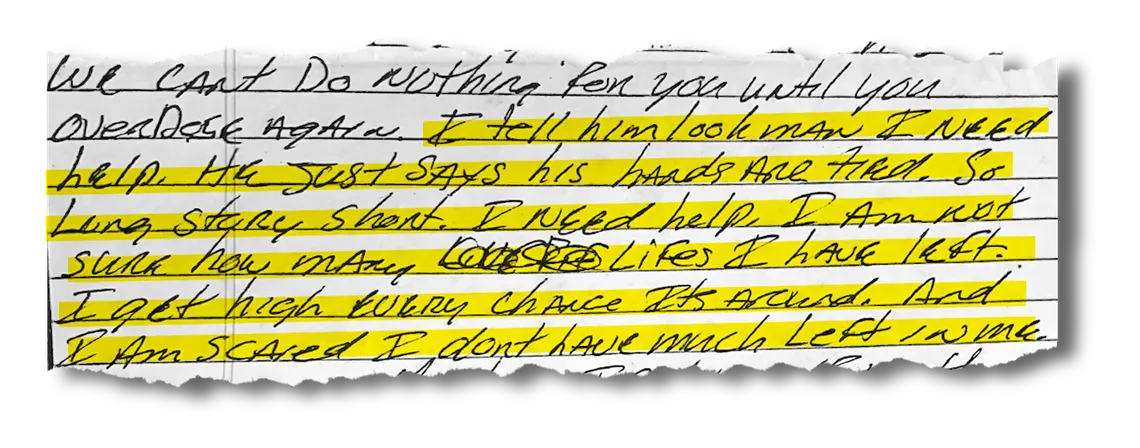
In a letter seeking legal help accessing treatment, a man describes his fear of dying after being denied medication.
In an email, a spokesperson for the department said any incarcerated person with an opioid disorder has access to institutional treatment programs, including individual and group counseling, and can be prescribed medication-assisted treatment, abbreviated MAT, if approved by their medical provider.
“Residents have access to short-term, intermediate and long-term programs, depending on need,” the spokesperson wrote. “The resident’s original conviction has no influence on access to treatment.”
However, Ketcherside’s family, and men incarcerated at prisons around the state, told The Marshall Project – St. Louis that access to treatment and rehabilitation services is rarely so straightforward.
“The way they live is so inhumane… they literally have to be on their deathbed before they get any kind of decent help,” said Ketcherside’s widow, Angela, in an interview with The Marshall Project – St. Louis. “ You expect that they’re gonna be safe, you know, now that they’re not on the streets. But they’re probably in more danger on the inside than they are out here.”
Last year, nearly 7,000 incarcerated people across the state were diagnosed with opioid use disorder, a spokesperson for the Department of Corrections said, compared with roughly 1,500 in 2024. (The spokesperson said the dramatic spike in part reflects a new assessment tool the department adopted last year to better screen for substance use disorder.)
In its budget request for fiscal year 2026, department officials reported that per person drug treatment costs between $6,500 and $14,200 a year. At that cost, officials estimated the department would be able to scale the MAT program from 121 people in 2024 to a total of 841 people by summer 2026. According to the department spokesperson, just under 3,700 people are currently receiving medically assisted treatment across the prison system. The spokesperson did not respond to questions about how the department is able to fund treatment at that scale.
In a 2025 amendment to its contract with Centurion, the healthcare provider for the prisons, the department noted it has nearly $7 million from the opioid settlement fund to spend on expanding the MAT program this fiscal year. The funding is he result of lawsuits against pharmaceutical companies and distributors, and are intended to be used to combat the opioid epidemic.
While the Department of Corrections has pointed the finger at incarcerated people, their visitors, and even mystery drone and catapult operators as potential culprits, the suit alleges that officials have done little to crack down on the role staff play in trafficking drugs through the prison system. Last year, multiple corrections officers in Missouri were charged with bringing drugs into prisons.
At Crossroads, the prison in Cameron, Missouri, where Ketcherside spent his final months, the main entrance had no overnight security for months at a time, the lawsuit alleges. Corrections officers and medical staff exploited this gap to profit off people with substance use disorder by “illegally smuggling drugs into the prison and selling them to incarcerated people,” according to the complaint.
In a prison system awash in drugs, the suit alleges incarcerated people are given a host of reasons they can’t receive treatment, including not having overdosed recently enough or not displaying severe-enough signs of addiction. In letters to attorneys on the case, multiple incarcerated people seeking legal help said they were denied treatment because they were not actively overdosing or in withdrawal.
The first time one man spoke with a nurse about treatment, “she stated that I was not currently withdrawing so, in so many words, they didn’t care,” he wrote in a letter provided to The Marshall Project – St. Louis. Another incarcerated man recalled a medical provider telling him, “We can’t do nothing for you until you overdose again.”
There are three primary medications for opioid use disorder: buprenorphine, methadone and naltrexone. The first two medications bind to opioid receptors to help stem cravings, while the third medication, which is more commonly prescribed in jails and prisons, blocks receptors but does not treat underlying cravings.
“Buprenorphine and methadone have decades of data showing their efficacy, and naltrexone does not meet that standard,” said Melissa Stein, a consultant who worked with Missouri DOC to develop its medically assisted treatment program.
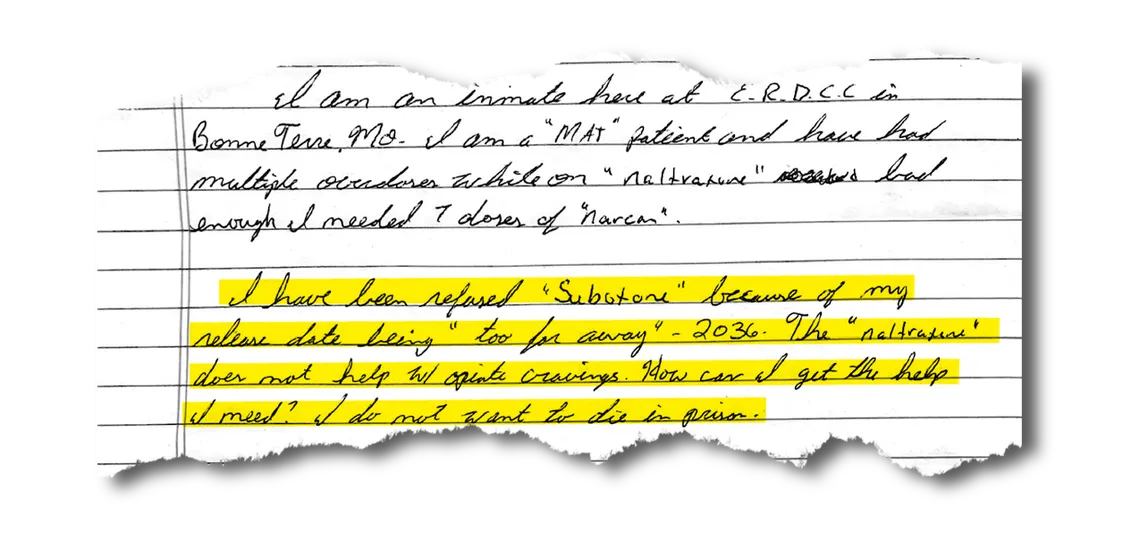
In a letter seeking legal help accessing treatment, a man describes being denied proper treatment for his substance use disorder because of how many years he has left in prison.
In letters, incarcerated people in Missouri prisons have reported being placed on naltrexone against their wishes, and forced to demonstrate negative side effects from the drug before being allowed to try other treatment options.
Stein said this approach is “ not in accordance with medical best practice, so we do not support that kind of policy.”
Prison officials denied Ketcherside’s request for medication two out of the three times he asked because he wasn’t close enough to his release date, according to prison records. His final attempt to access MAT was rejected, despite his extensive history of opioid use and multiple overdoses, because in an evaluation that lasted less than 15 minutes, mental health staff determined Ketcherside was “not intending to use opiates” after he said he was trying to stick to K2, a name for synthetic cannabinoids, instead.
“Offender repeatedly said that this ‘would save my life!’” the mental health evaluator wrote in the appointment note. “Offender claimed that this was a service he needed … but did not meet criteria due to his not using opiates since overdose on 7/2/2024.”
ACLU Staff Attorney Joseph Longley said these arbitrary reasons for denying care are both unconstitutional and disability discrimination. “There’s really no excuse,” he said, “and them not providing it anyway is such a clear example of deliberate indifference to the medical needs of people with opioid use disorder.”
The risk of addiction-related death isn’t just from overdoses. Opioid withdrawl, often triggered by placement in solitary confinement, is a medical emergency and can drive people to suicide or self-harm.
In a letter to Fessler at the start of last year, Brandon Church described being taken off his medication for opioid use disorder while in solitary confinement at Jefferson City Correctional Center, in Missouri’s capital city. He begged for assistance to get back on medication, and said his repeated medical requests had gone unanswered.
“I’m addicted to opioids and self-harm. When I was on the medication it was so much better, for once in my life I felt normal. My cravings were gone,” the 34-year old wrote. “I would really like to make it home. … Have a happy new years and god bless.”
Fessler never got a chance to respond. Two weeks later, prison staff found Church hanging by his neck from a bar in his cell, according to his autopsy report.
Private health care providers have a well-documented pattern of creating barriers to treatment access in prisons, experts said, and Missouri is no exception. Centurion Health is a contractor that is incentivized to operate with profit margins — not people’s health — as the top priority, experts argue.
“The less medication they prescribe, the more money they save in their contract, the more profit they make their investors,” said Dr. Fred Rottnek, a professor at St. Louis University School of Medicine and consultant with Policy Research Associates on access to substance use treatment in prisons.
More often, the department responds to substance use with punishment, the suit alleges. Possession or use of an intoxicating substance is a violation of Rule 11 in Missouri DOC’s Offender Rulebook, punishable by the most severe range of sanctions: An incarcerated person can be confined to their cell, forced to work extra hours, have their wages cut or be placed in solitary (where, according to multiple reports, drugs are still available). Violations can also impact a person’s eligibility for rehabilitation programs and even their date of release. Some incarcerated people have reported not being able to access treatment because they were too far away from their release date, only to have that date pushed further back because they were caught using drugs.
“My drug use resulted in violations that resulted in extending my stay,” one man wrote in a January 2025 letter to attorneys on the case. “MODOC has refused to help me and continued to punish me for my substance abuse, addiction, and mental health conditions.”
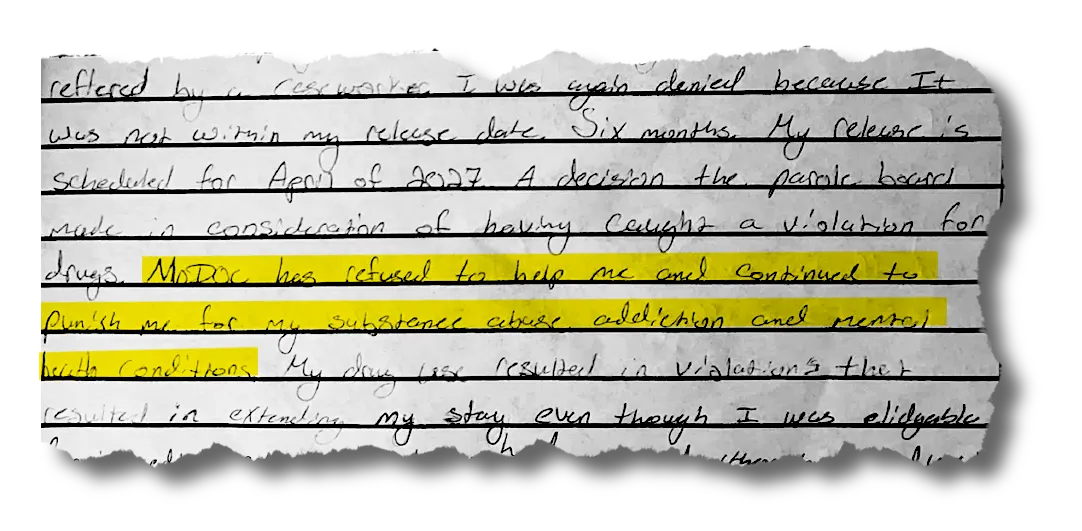
In a letter seeking legal help accessing treatment, a man says the state has punished him for his addiction, rather than helping him.
A department spokesperson declined to comment on the range of sanctions for substance use, and said in an email that staff refer people struggling with addiction to treatment providers who can connect them with “supportive services” such as counseling.
“The current awareness campaign aims to help de-stigmatize addiction and encourage residents of our facilities to seek help,” the spokesperson wrote.
The prisons do offer behavioral health programming as one response for those caught using drugs. But experts say the state’s substance use program is currently insufficient to meet the needs of its incarcerated population. A combination of cost, understaffing and stigma has kept the department’s progress on improving treatment options to an arthritic pace, Rottnek said. And in letters to attorneys on the case, incarcerated people who did enter treatment wrote that the programs they were offered didn’t work.
“I’ve done several programs and even just completed Hustle 2.0,” one man wrote, referring to a behavioral health rehabilitation program offered by the prison. “However, I can’t shake or beat this on my own. I realised this the last time I woke up with my celly giving me mouth to mouth. He was crying and said, ‘Bro. You were dead.’”
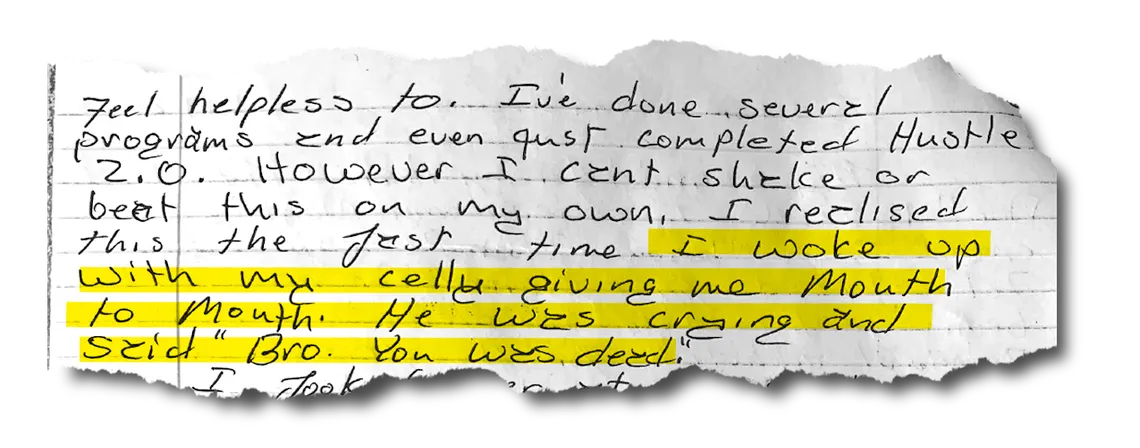
In a letter seeking legal help accessing treatment, a man recounts his realization that he can’t beat addiction on his own and needs medical treatment.
In addition to monetary relief for Ketcherside’s widow and the children who considered him a father and friend, the lawsuit calls for the court “to punish defendants and to deter them” from ignoring the rights of the people in their care. Fessler, the lead attorney on the case, said she hopes the lawsuit will “demonstrate to the DOC and to Centurion the consequences of not focusing on this MAT program and really making it effective and accessible for everybody who has opioid use disorder in prison.”
Fessler believes MAT access could be life-saving. She pointed to the story of Colby Rey, who has been incarcerated in Missouri prisons since 2022, as an example of what can happen when addiction is properly treated. After two years of begging the prison system for help, and three overdoses that sent him to solitary confinement, his life behind bars dramatically improved when he was put back on the buprenorphine treatment he was receiving prior to his incarceration. The DOC only relented after Rey sought legal recourse, working with Fessler to draft a demand letter to the prison.
Ketcherside’s widow, Angela, is hoping the lawsuit will bring about necessary reforms, so incarcerated people won’t suffer the same fate as her husband.
“It all comes down to the fact that he was their responsibility,” she said. “And if they had done their job properly, he’d still be here.”


{kind=link}